WHAT IS OCD?
OCD: A LIFE-LONG BATTLE
1.5% of women and 1.0% of men worldwide suffer from OCD, a chromic neurodevelopmental anxiety disorder characterized by recurring, intrusive thoughts or images that cause extreme distress and anxiety – and the compulsive need to carry out repetitive, ritual acts to reduce that anxiety.
The WHO lists anxiety disorders, including OCD, as the sixth largest contributor to non-fatal health loss globally. Currently 9.45 million people live with moderate or severe OCD in Europe, the US, Japan and the UK.
A safe, fully effective pharmaceutical therapy still does not exist.
STIGMA, SECRECY, SEVERITY
Despite being so prevalent, the underlying neurological and hormonal mechanisms that cause OCD remain poorly understood. Current front-line treatment is demanding, arduous, costly and time-consuming. Recidivism is high. Of people diagnosed with OCD:
- 96% suffer from moderate to severe versions
- 50%+ experience impairment so serious they are unable to lead normal lives
- 40–50% remain resistant to current treatments
UNMET NEED, NEW DEVELOPMENTS
There is no safe, highly efficacious pharma medication for OCD, despite 50% of diagnosed patients being seriously impaired and unable to lead uninterrupted lives.
SSRIs have an overall efficacy of < 50%. They can be effective at reducing OCD anxiety, but they fail to treat the compulsive mechanism in OCD.
The lack of pharmaceutical options can lead to some physicians prescribing off-label medication with serious side effects (from second-line central nervous treatments like atypical neuroleptics or antipsychotics like Haloperidol).
FRONT-LINE TREATMENT
Today’s front-line treatment is Cognitive Behavioral Therapy or CBT, and specifically ERP (exposure and response therapy). ERP is a systematic program of re-conditioning developed specifically to treat OCD. Through continuous training it gradually breaks down the connection between fear and compulsion, bringing them under conscious control and eventually eliminating both. ERP can work well – but it is demanding, costly and time-consuming. Relapse is common, patients are taught as part of the therapy that although their specific fear may be successfully overcome, the same pattern of obsession and compulsion could resurface around a different fear, even years later, particularly in high-stress situations.
ALLOPREGNANOLONE: THE KEY TO COMPULSION?
A key factor in the lack of effective pharma therapy is the absence of a treatment that targets the compulsive mechanisminherent in OCD. The obsessive fear and anxiety element can be reduced somewhat through SSRIs. Yet that can only ever be half the story for a condition driven by two symbiotic motors – obsession and compulsion.
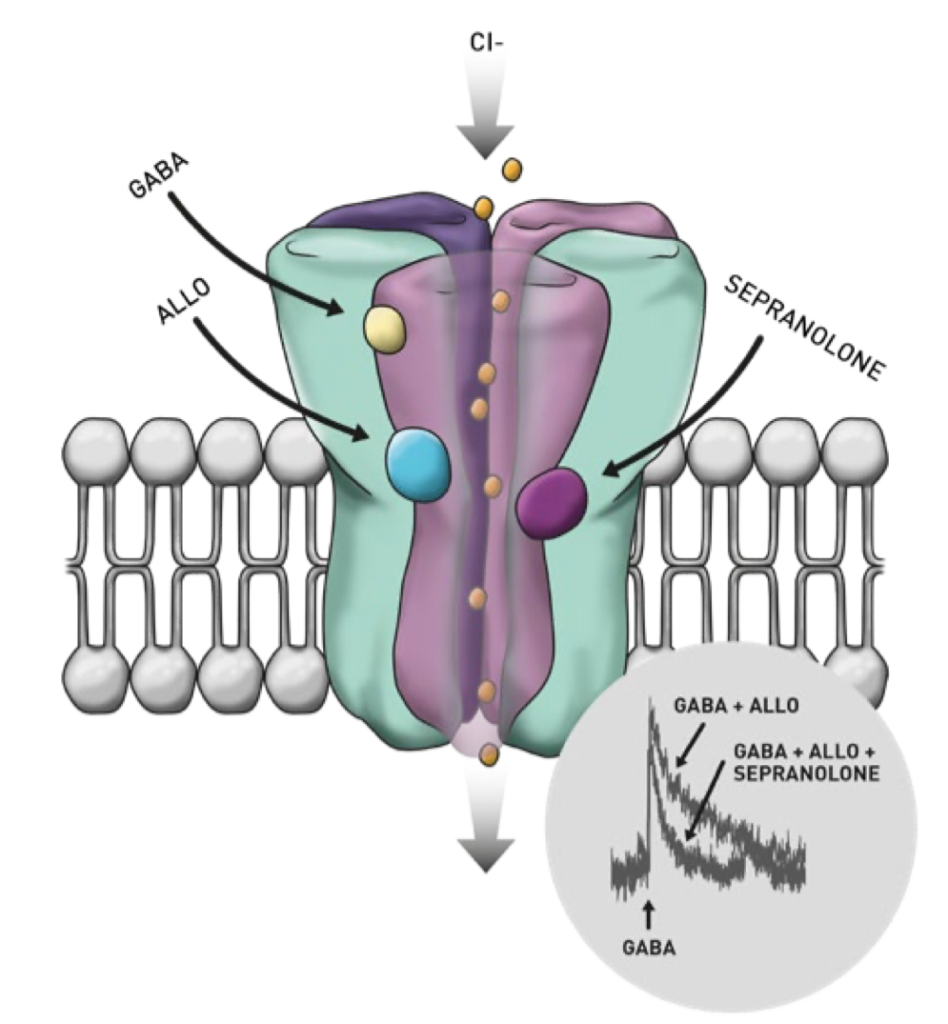
New research is now pointing towards the role of one of the brain’s most potent neurotransmitters – Allopregnanolone – in triggering compulsion.
And a treatment that modulates and inhibits the negative effects of this substance already exists…